– An Approach to Reopening the Economy without Pandemic Resurgence
By Winston Ma and Clemens Szyperski
Introduction
Since social and physical distancing, self-quarantine and isolation began to be put in practice, the coronavirus pandemic curves have started to flatten according to how stringently they are implemented in the states around the country. As the situation improves the debate about lifting restrictions heats up again: should we allow the economy and industries to continue their free falls until vaccines become widely available, or reopen the country and risk resurgence of the pandemic? Can we reignite the engine of the country’s economy and steam ahead with healthy growth while contain the pandemic effectively? Good economic policy calls for good pandemic control policy.
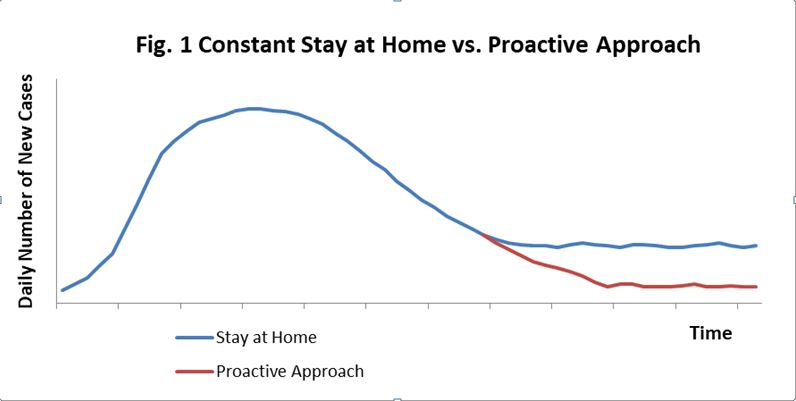
Tough problems are usually not solved by direct assaults; they dissolve if you put proper conditions in place. The basic strategy we need is the same as that used for fighting wildfires. After the flames have passed, firefighters conduct mop-up operations, checking all the hot spots and knocking each and every one of them down, leaving no chance for the fire to resurge. We would like to propose a similarly proactive pandemic management approach to ensure that we can we resume normality and further lower the number of cases of infection as we progress forward (see figure 1).
In this proposal we present the preconditions required for reopening the country, the critical measures that must be taken in order to keep the pandemic under control and the key pillars necessitated to ensure the success of these measures.
Two Preconditions for Returning to Normality
In order to keep coronavirus spread under control while reopening the economy, we need to have two necessary preconditions in place:
1. Limited number of new cases
To reopen the economy without a resurgence of cases of infection, we need to maintain current social distancing, self-quarantine and isolation until daily new cases drop to a manageable level. We have been underreporting coronavirus cases since virus testing has been limited in capacity and biased toward those who are symptomatic. Some extended regional samples, which include asymptomatic cases, showed that the underreporting of cases may be by a factor of 50+ indicating that the real picture of the pandemic is far worse than what has been reported based upon existing schemes of testing. Regular random sample testing must be conducted to monitor the progress and no region is allowed to reopen its normality until its pandemic reaches the manageable level. Given the fact that the severity of the pandemic and the containment capacity vary greatly between regions, it is very likely that each region will achieve the manageable level at different times, requiring enforced travel restrictions between them.
2. Adequate testing, contact tracing and isolation capacity
Once a region’s pandemic falls to the manageable level and it returns to normal work and life, extensive and constant operations must be kept to mop up sporadic cases and small clusters of outbreaks. A region achieves its manageable level of the pandemic at which each and every suspected case is tested without delay, contact tracing is accomplished effectively and timely, and all infected are placed in quarantine or hospitalized.
Four Critical Measures
Keeping the epidemic at bay requires a comprehensive set of measures and these measures must be operationalized, tested and be measurable before any region is reopened.
1. Social Distancing and Hygiene
Social distancing has been effective in containing coronavirus spread. In addition to requiring citizens to keep a 6 feet distance wherever possible, sanitizers should be available in all the public places. Face masks should be used when working in closed spaces for long period of time, UV lights and disinfectant sprays or vapors, which are less labor- and time-intensive, should be used regularly to eliminate the virus in wide spaces.
Given the fact that situations vary between workplaces, experts should be sent to help identify, establish, and apply social distancing best practices for various workplace scenarios.
2. Coronavirus RNA, Antibodies and Antigens Testing
Each and every suspected case must be tested!
So far, there are three types of COVID-19 tests detecting its RNA, antibodies, and antigens.
While RNA testing offers the benefit of detecting virus existence in a person, it could produce a false negative because viruses are mostly present deep in the lungs and swab sampling may fails to pick them up and also because the disease progresses at different clinical stage (Wikramaratna et al, 2020). RNA testing will also be negative once the virus has been cleared from the body. Ab testing, though it has several days delay, serves as an indicator for infection (IgM) and post-infection immunity (IgG). Additionally, Ab testing is fast, low-cost, as easy to use as a pregnancy test at home, and, therefore, more suitable for regular testing in broad scales. We propose that coronavirus RNA and antibody (Ab) testing should be conducted together as we work toward returning to normality.
We should conduct Ab testing for coronavirus close contacts and regular screening for the entire population. The benefits of such a scheme of testing include: 1) Accurate information of the speed and degree to which the populations have been infected and have developed immunity; 2) Capture suspect cases – the infected cases which are still at contagious stage and the asymptomatic virus carriers; 3) Comfort those who have already gained post-infection immunity (with IgG Positive) and encourage them to work, live with normalcy and donate anti-COVID-19 plasma to help those who suffer from severe infection; and 4) Reduce future workload of close contact tracing as increasing number of the contacts gaining post-infection immunity.
Researchers reported that serological Ab levels varied between pneumonic SARS patients and asymptomatic cases (Wilder-Smith et al 2005) and this may be true among COVID-19 cases. On the other hand, Ab levels are dynamic in infected cases and those who have cleared virus seem to have higher IgG titers than those who still carry the virus (Jin Y et al, 2020). Therefore, the Ab testing panel should be designed to achieve several objectives: 1) capture the cases of acute infection that are still contagious. These cases are IgM positive with or without very low levels of IgG. A low level of IgG – “Recovering IgG Level” – needs to be established to signify the stage at which the acute infection cases are virus-free; 2) identify those who have completely recovered from the infection. A high level of IgG – “Clearance IgG Level” – should be determined through research and experiments to signify absence of virus and strong post-infection immunity. Further studies, however, are required to examine the Ab level below which virus reinfection or “re-activation” could take place; and 3) find asymptomatic virus carriers, which show a low serological IgG level. Whether the IgG levels among asymptomatic virus carriers differ from the “Recovering IgG level” among acute infection cases needs to be further investigated.
IgM testing should be set at the lowest threshold possible – most sensitive – for the purpose of catching those who have caught the virus and are contagious early on. Those who are still IgM positive but have cleared the virus will be excluded through IgG testing at an appropriate titer.
IgG testing should be set at two thresholds: 1) A high IgG threshold needs to be established in testing to signify strong post-infection immunity with negative virus presence. 2) A low IgG threshold should be set to capture patients who have cleared the virus after an acute infection, asymptomatic virus carriers, and those who have developed lower level of IgG and are at risk of re-infection.
All those who have tested High IgG negative should be included in the next round of Ab testing.
Proper thresholds for IgM and IgG testing should be established through clinical investigation as the followings:

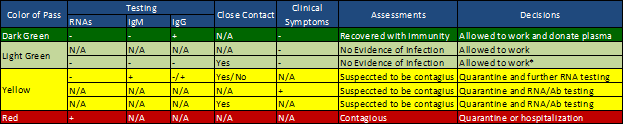
All testing data should be gathered and analyzed by centralized data systems for policy and guideline adjustments. The outcomes of the testing can be registered and shown on mobile apps as “passes” for the person’s mobility permissions:

So far, scientists have detected thousands of mutations of the new coronavirus. Such mutations represent constant changes in RNA sequences and virus antigenic epitopes and, therefore, indicate the possibility of the need to renew PCR primers and antigens for testing. We need to monitor the divergences between clinical data and testing results and between RNA and Ab testing.
The antigen test is the third type of test to be authorized by the FDA. Although, as a serological immune test, it is also fast, low-cost, and easy to use, serological antigens won’t be detectable until the virus breaks into the blood stream from the respiratory system and produces detectable amounts of copies. Hence, it will likely lag behind PCR-based RNA tests, which take samples directly from the respiratory system and amplify the signal of the virus by replicating its RNA, and also behind the antibodies, whose production escalates as the body responds to the virus’ challenge. Clinical investigations are needed to understand the dynamics of the serological antigens and its relation to asymptomatic, mild, moderate and severe cases.
3. Mop-Up and Hot Spotting
Each and every suspected case and close contact must be checked and tested!
3.1 Examine Suspected Cases
Incentive and convenience must be provided to encourage those who manifest Covid-19-like symptoms to come forward and request for testing, quarantine, or hospitalization. To encourage citizens’ participation, the costs of testing, quarantine, and hospitalization must be covered by public funds and their jobs should be preserved wherever possible through public assistance to their employers.
3.2 Contact Tracing
Contact tracing organizations need to be established at various levels, with legal power for investigation and data systems to support their operations. Contact tracing personnel should be required to work as case workers with every person who has been tested positive for coronavirus. Close contacts in the past two weeks have to be traced and tested. If positive cases are identified in these contacts, a cascade of further contact tracing should be conducted.
We will encounter cases of people, who have already recovered with negative virus test and therefore, both coronavirus RNA and Ab testing should be used:
3.2.1. A close contact who tests High IgG Positive should receive Dark Green pass and be sent back to normal work and live.
3.2.2. A close contact who tests both IgM and IgG negative and has already passed IgM seroconversion time after the date of contact should be allow to work and live with normalcy.
3.2.3. A close contact who tests IgM positive or/and Low IgG positive but High IgG negative should be placed in quarantine until RNA tests negative.
3.3 Body Temperature Measuring in Public Places
To reduce virus spread in public places and capture suspected sources of infection, body temperature must be measured before entering public places, in addition to checking the color of the pass on each and every person’s mobile device.
3.4 Regular Testing Requirements in Workplace
In addition to body temperature measuring in workplaces, employers should be required to renew their employees’ mobility passes on a regular basis through Ab testing.
4. Quarantine and Treatment
All those, who are suspected to be contagious (YELLOW or RED pass in their mobile apps), should be placed in quarantine or hospitalized. Quarantine laws should be established so that designated forces get to randomly check passes in public space and employers are required to repeat pass-checking on a regular basis. If anyone violates quarantine rules before their pass turns to GREEN, a significant penalty must be given for each violation. On the other hand, incentives such as costs of quarantine or/and hospital stay and living expenses should be provided from public funds so that incidents of violation can be minimized.
The Key Pillars
The four critical measures described in this proposal require support from legal, organizational, technological and financial aspects. These key pillars should be funded by federal government, guided by CDC and carried out by local government agencies.
1. Contact Tracing Organizations
We need organizations of case workers to work with everyone who has been tested positive for coronavirus to trace their close contacts, the public spaces they visited and the public transportation they’ve used in at least the past two weeks. These organizations will be managed by local governments under CDC’s guidance. The case workers can be hired from the growing number of unemployed Americans and trained to conduct contact tracing. It is crucial that these organizations should have legal backing and enough technological support to conduct contact tracing effectively.
2. Data Platforms and Apps
Centralized data platforms should be developed for efficient data registration, dispensing, and utilization. Mobile apps should be used to issue and renew passes of colors. Green passes must be required for travel and work during this recovery period. (For some elaboration on such a platform and app approach, see the section of Tracing Support.)
3. Rules and Laws for Information Acquisition and Quarantine Enforcement
A new set of rules and laws need to be established and enforced to support pandemic monitoring, contact tracing, quarantine enforcement, and, of course, privacy protection. Penalties must be given for each and every violation.
4. Free Testing and Free Treatment
We would like to propose that financial assistance such as costs for testing, quarantine, hospitalization, and cost of living due to quarantine and hospitalization should be covered by governments. Such assistance provides citizens adequate incentive to follow quarantine rules.
Tracing Support
Technology can be very beneficial when seeking to automate or at least greatly ease contact tracing. Some countries are using technology, such as location services of cell phones (and proximity data of cell phones relative to each other) from service providers or facial recognition applications running over camera feeds from public locations. In countries where such blunter use of technology is illegal and broadly rejected by the population, more sophisticated approaches are needed.
1. Phone location services
Practically all modern smartphones can locate their own position with fairly high accuracy using a combination of technologies, from cell triangulation to GPS. Users can decide which apps should have access to that information. If a tracing app is to be successful, users need to be convinced that the app won’t disclose their location history.
2. Proximity
If two phones report their present location to a suitable service, the service can determine whether those two phones are in proximity at any particular point in time. In addition, phones can detect proximity based on things like Bluetooth ID broadcasts or proprietary protocols like Apple’s AirDrop. These latter mechanisms could be leveraged, under close wraps, if Apple and Google collaborated, which seems possible based on recent announcements.
3. Contact Detection
Phones that detect that another phone is (likely) within proximity will report an ID for the other phone that is unique to the detecting phone and the time of detection. Neither the detecting phone nor any app on it can use such IDs to trace other people. However, a trusted cloud service would be able to correlate based on such IDs. If both phones had active apps already, then the apps would just self-report their location to the cloud service that would then proceed to correlate as before.
4. Alerting
If the tracing service detects that a person has been in proximity to someone else who is now known to be possibly infected, the service considers the status of both the person to be alerted and of the possibly infected person. For instance, if the person to be alerted is known to be immune (“dark green”), the encounter can be ignored. Or if the possibly infected person has a positive RNA result (very likely contagious), the service can calculate back to see whether the encounter was before that person became contagious. If, based on such calculations, the service determines that the encounter needs to be traced, it issues an alert.
The alerted user can be told when they got close to someone possibly infected, without revealing who that person was, which allows the app to calculate a safe self-quarantine timeframe. (The alerted user could also be told the place where that encounter happened. However, the more information is revealed, the broader the set of cases where the alerted user can tell who it was that possibly infected them. Any such “finger pointing” can trigger adverse social behavior that should be avoided.)
5. Status Adjustment
As an alert was raised, the app’s color would change to “yellow”. The service does not need to “tell” the alerted user on some authorities. The app can allow for a volunteer “report myself” button, but mostly the app’s change in status color would allow for “door checks” in public or workplaces.
6. Tamper-Resistant Status
While the simple color coding allows for easy interpretation of an app’s status, it is important that the status cannot trivially be forged. Things like showing a screenshot from before the color changed, say from green to yellow, should be prevented. The easiest way to do that is to have the app show both the color code and a QR code that encodes an encrypted ID and timestamp. Anyone scanning that QR code can get confirmation that the color code did indeed come from the cloud service and is currently valid.
Such techniques preserve anonymity and don’t prevent all attempts of misrepresenting someone’s status. For instance, someone could just show another person’s phone. Instead of combatting such cases with technology, it would seem advisable to rely on legal measures. For instance, there could be a stiff penalty for people who get themselves into a public event by misrepresenting their status.
7. Distancing Notification
Optionally, an app could warn a user that there is someone with a “yellow” or even “red” status nearby but not yet in proximity. This information could be used by the warned person to actively distance themselves. Such an option could create anxiety or even panic though and should be considered carefully.
8. Opt-In
It would be advisable to allow users to moderate how much they want the app to do automatically. In the most extreme case, the app would ask the user every time it would otherwise send some information to the service and the user can decide to allow that – or not. While any such freedom of choice will reduce the total precision of the service, it should help boost buy-in. That is more important than precision since the goal is broad coverage and statistically effective tracing.
Summary
The authors believe that we will be able to contain the pandemic and resume economy growth and normalcy of our live and work, without the need to attain “herd immunity” as a precondition, as long as we take this proactive approach of keeping social distancing, testing for coronavirus, contact tracing, and quarantine enforcement. To ensure the effectiveness of this approach in keeping the pandemic under control, we need to put together a comprehensive set of legal, organizational, technological, and financial support before reopening any region. A close monitoring of the situations must be kept at all levels. Should any region open up prematurely or fail in implementing the approach we simply send the entire region back to isolation and start all over again.
Key References
Jin Y et al. Diagnostic Value and Dynamic Variance of Serum Antibody in Coronavirus Disease 2019. (https://www.ijidonline.com/article/S1201-9712(20)30198-3/pdf)
Wikramaratna P et al. Estimating False-Negative Detection Rate of SARS-CoV-2 by RT-PCR. (https://www.medrxiv.org/content/10.1101/2020.04.05.20053355v2)
Wilder-Smith A et al. Asymptomatic SARS Coronavirus Infection among Healthcare Workers, Singapore. Emerg Infect Dis. 2005 Jul; 11(7): 1142–1145. (https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3371799/)